
Transcribed Image Text from this Question
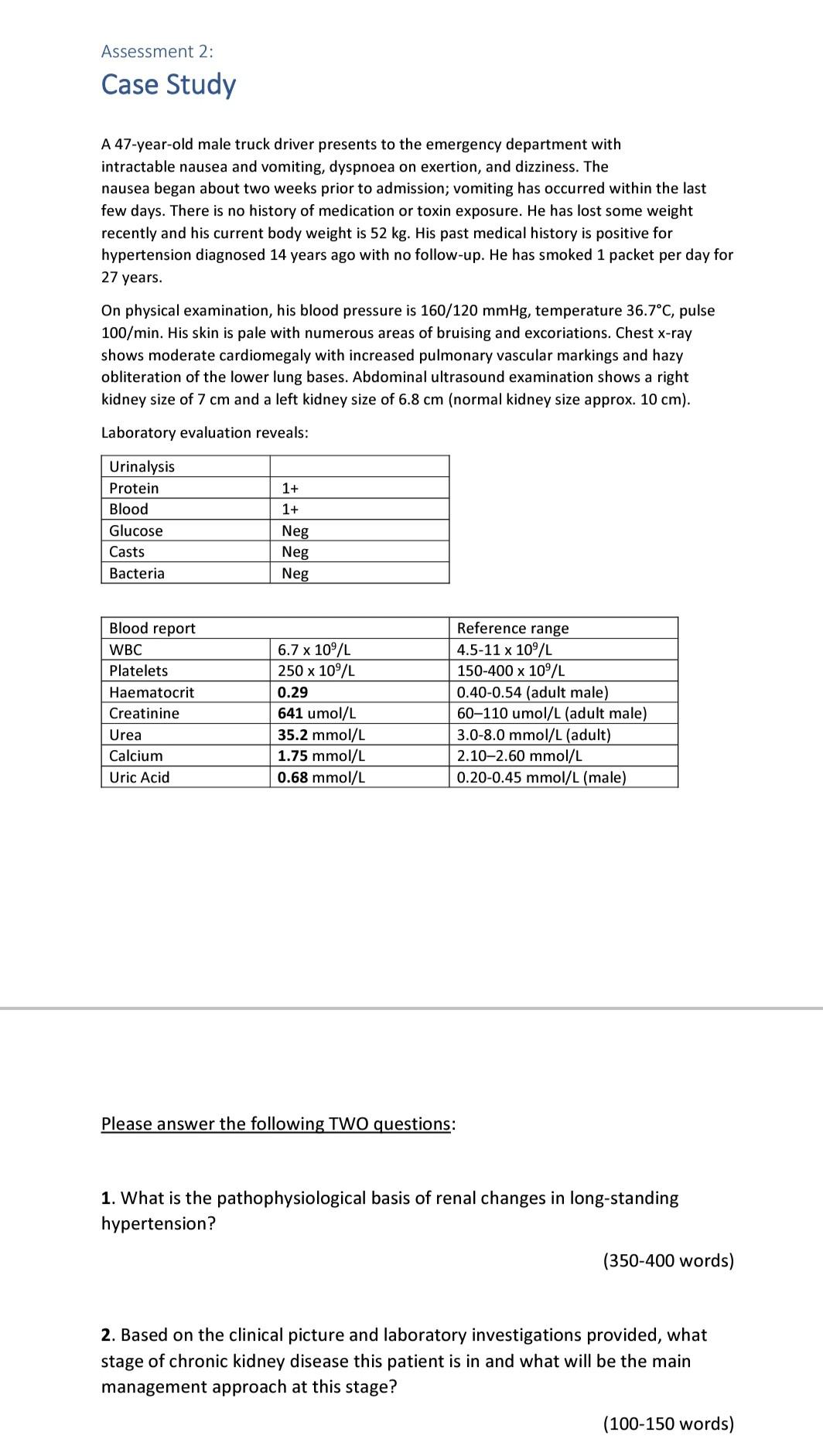
Assessment 2: Case Study A 47-year-old male truck driver presents to the emergency department with intractable nausea and vomiting, dyspnoea on exertion, and dizziness. The nausea began about two weeks prior to admission; vomiting has occurred within the last few days. There is no history of medication or toxin exposure. He has lost some weight recently and his current body weight is 52 kg. His past medical history is positive for hypertension diagnosed 14 years ago with no follow-up. He has smoked 1 packet per day for 27 years. On physical examination, his blood pressure is 160/120 mmHg, temperature 36.7°C, pulse 100/min. His skin is pale with numerous areas of bruising and excoriations. Chest x-ray shows moderate cardiomegaly with increased pulmonary vascular markings and hazy obliteration of the lower lung bases. Abdominal ultrasound examination shows a right kidney size of 7 cm and a left kidney size of 6.8 cm (normal kidney size approx. 10 cm). Laboratory evaluation reveals: 1+ 1+ Urinalysis Protein Blood Glucose Casts Bacteria Neg Neg Neg Blood report WBC Platelets Haematocrit Creatinine Urea Calcium Uric Acid 6.7 x 10°/L 250 x 10°/L 0.29 641 umol/L 35.2 mmol/L 1.75 mmol/L 0.68 mmol/L Reference range 4.5-11 x 10°/L 150-400 x 10°/L 0.40-0.54 (adult male) 60-110 umol/L (adult male) 3.0-8.0 mmol/L (adult) 2.10-2.60 mmol/L 0.20-0.45 mmol/L (male) Please answer the following TWO questions: 1. What is the pathophysiological basis of renal changes in long-standing hypertension? (350-400 words) 2. Based on the clinical picture and laboratory investigations provided, what stage of chronic kidney disease this patient is in and what will be the main management approach at this stage? (100-150 words)
(Visited 12 times, 1 visits today)


