Audit Report 1.1 Hospital Services
LOCATION Inpatient, Hospital PATIENT: Dana Obright
ATTENDING PHYSICIAN Marvin Elhart, MD REASON FORADMISSION: Congestive heart failure.
The patient is an 82-year-old Caucasian female who wasgetting ready to go to bed tonight and felt sudden shortness ofbreath She had no chest pain, neck, or jaw pain. She could not takea deep breath, She presented to the emergency room where a chestx-ray was obtained, and she was in florid pulmonary edema, and herblood pressure was 180s-190s/110
The patient has been having exertional dyspnea forsome time. She Usually sees Dr. Noonar. She recently had apacemaker placed for sick
sinus syndrome.
Thie patient had a recent echocardiogram, which showednormal left ventricular systolic function with severe mitralregurgitation and tricuspid regurgitation with moderate pulmonaryhypertension
PAST MEDICAL HISTORY
1. Hypertension
2 History of atrial fibrillation
3. Thoracic aortic aneurysm.
4 Hysterectomy
5. Bilateral cataract surgery. ALLERGIES No known drugallergies
SOCIAL HISTORY. Retired, lives in Manytown. She iswidowed. She denies any alcohol or smoking,
FAMILY HISTORY Positive for cancer and diabetes. Shehas an aunt who had breast cancer, otherwise negative
MEDICATION
1. Clonidine patch 0.2
2. Vasotec 10 mg qd.
3 Premarin 0625 mg d.
4. Labetalol 100 mg bid
REVIEW OF SYSTEMS: General Pale. No fever, chills, ornight sweats No change in weight or loss of appetite. ENT Negative.Eyes Negative Cardiovascular: No claudication. Occasional leg edemaThe rest as mentioned in the HPI GU Negative. GE Negative. Skon:Negative Neuro Negative. Musculoskeletal: Occasional arthralgias,otherwise negative Respiratory: Cannot get her breath
PHYSICAL EXAMINATION: saw the patient after shereceived 1 mg of Bumex and after she diuresed more than 1000 cc.She was lying in bed not in any distress. Blood pressure went downto 102/90s. Heart rate 80s to 90s per minute Respirations 22 perminute She is pale and afebrile. There is increased jugular venouspressure and mild neck vein distention. Lungs show good air entrybilaterally with crackles in the bases. Abdomen: Obese, nontender.No organomegaly Extremities: 1+ edema. She has a Foley catheter,which has light urine
LABORATORY STUDIES: All her labs including CBC, basicmetabolic panel, and troponin today were negative
CHEST X-RAY Cardiomegaly and florid pulmonary edemawith edema in
the right transverse fissure
IMPRESSION
1. Congestive heart failure, multifactorial. Probablyshe has left ventricular hypertrophy and also mitral regurgitationthat tipped her over the edge
2. Hypoxic with saturations of 86% on room airsecondary to pulmonary edema
PLAN: I will give her another 0.5 mg of Bumex IV. Wewill repeat her labs at 9 including troponins The patient does notusually use salt in her diet, but we will fluid restrict her for1500 c.
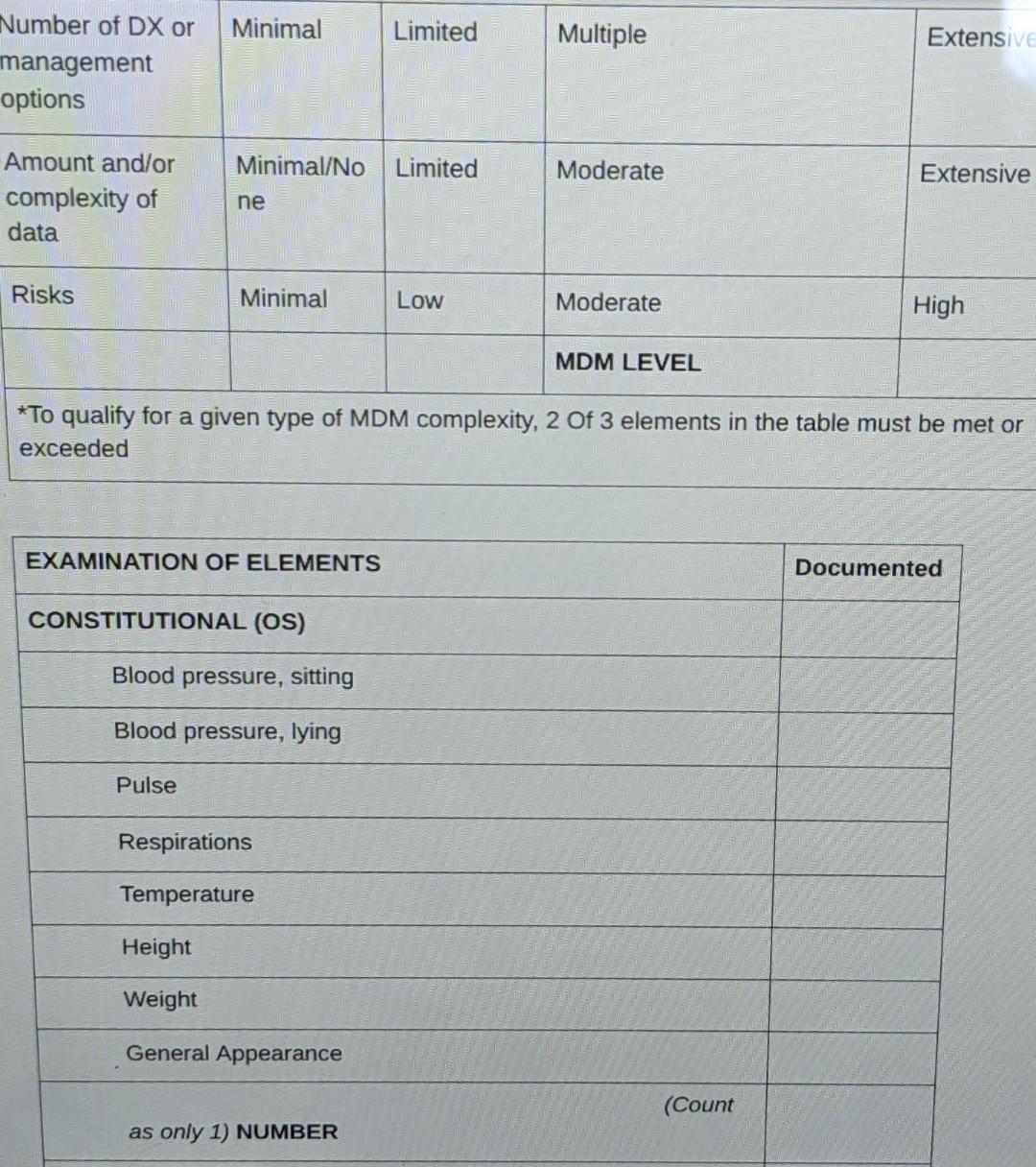
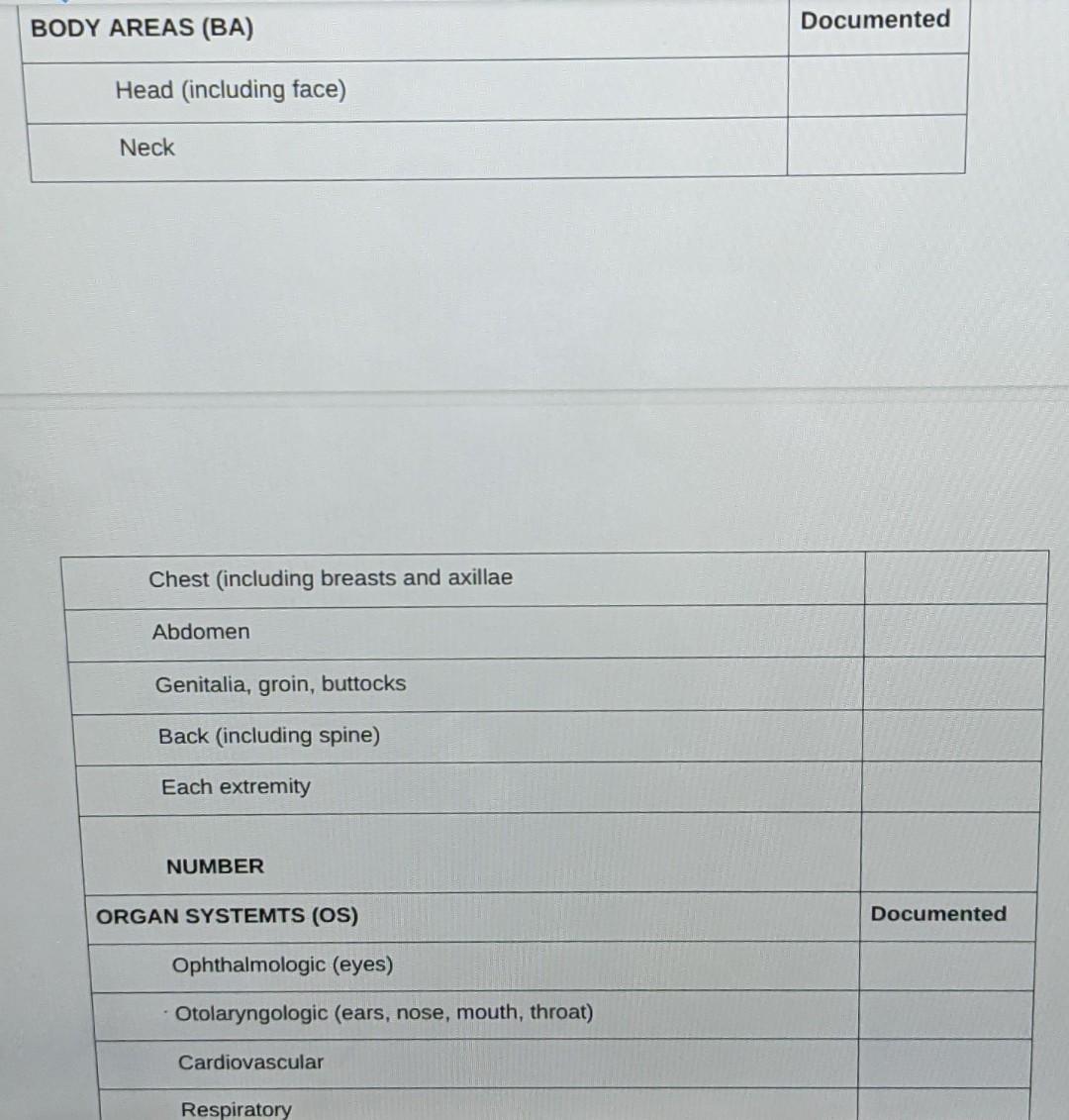
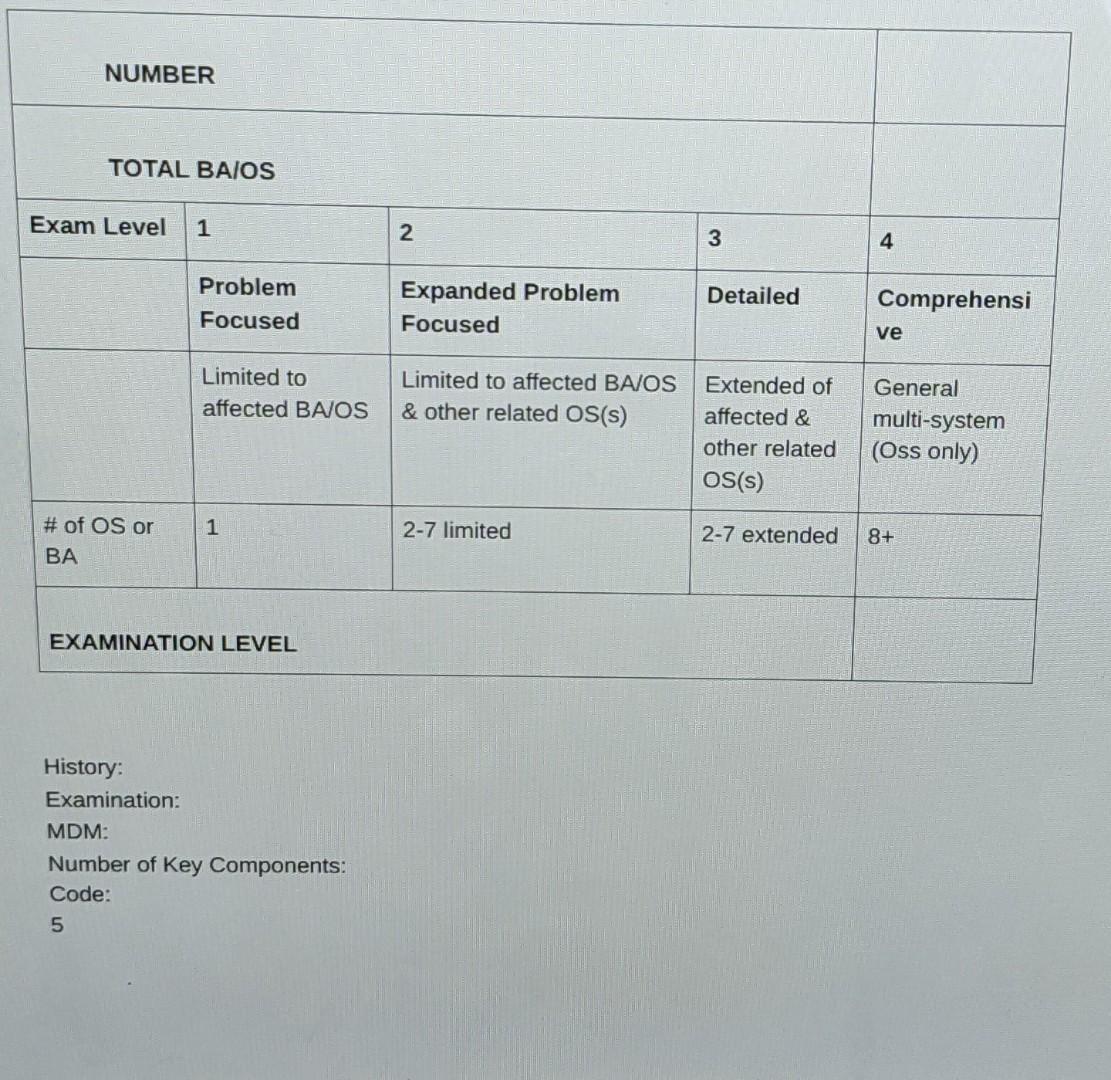
One of the following codes is reported incorrectly forthis case Indicate the incorrect code
PROFESSIONAL SERVICES: Evaluation and Management,99222
ICD-10-CM DX: Congestive heart failure, 150.9
INCORRECT CODE: N/A
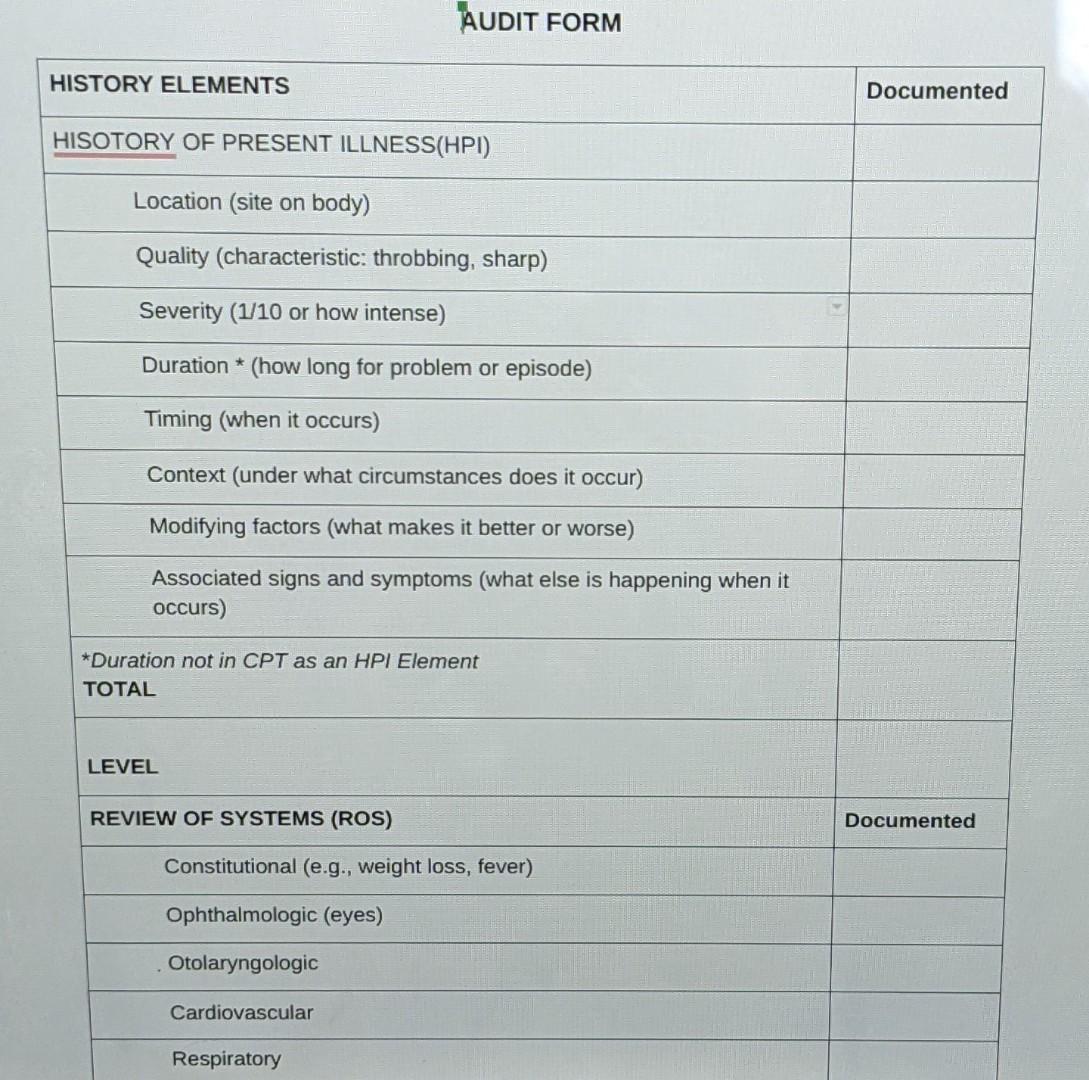
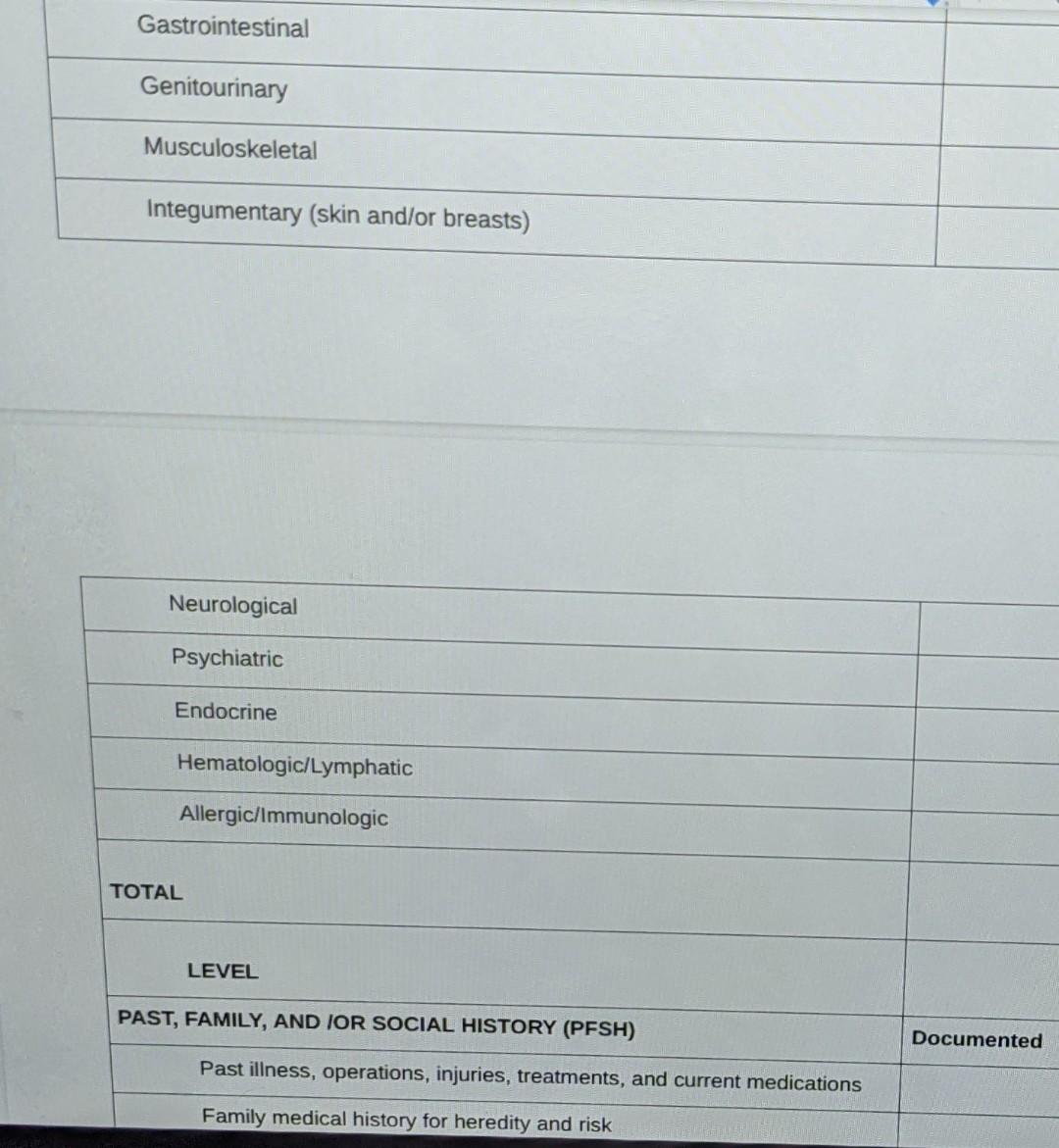
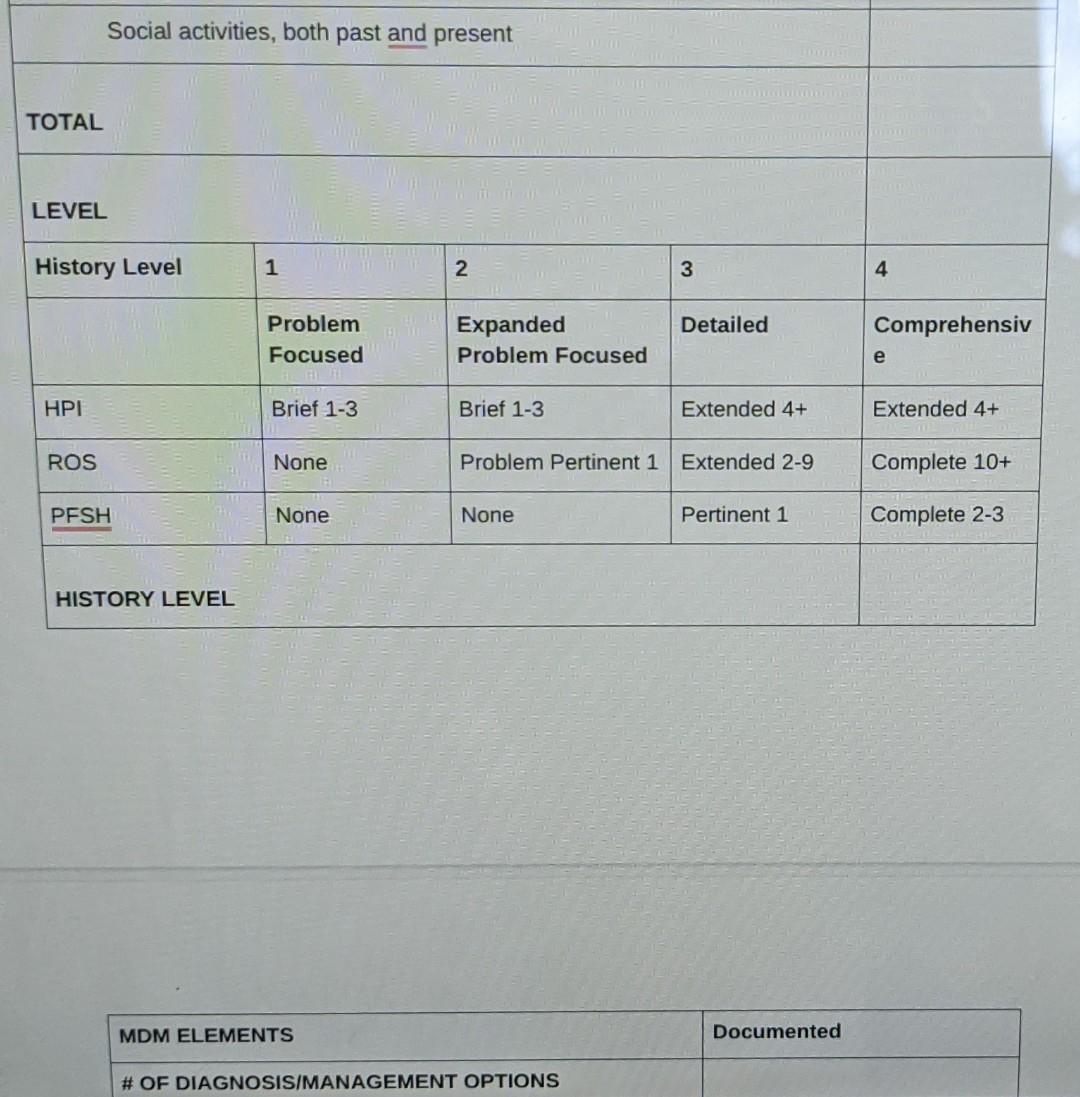
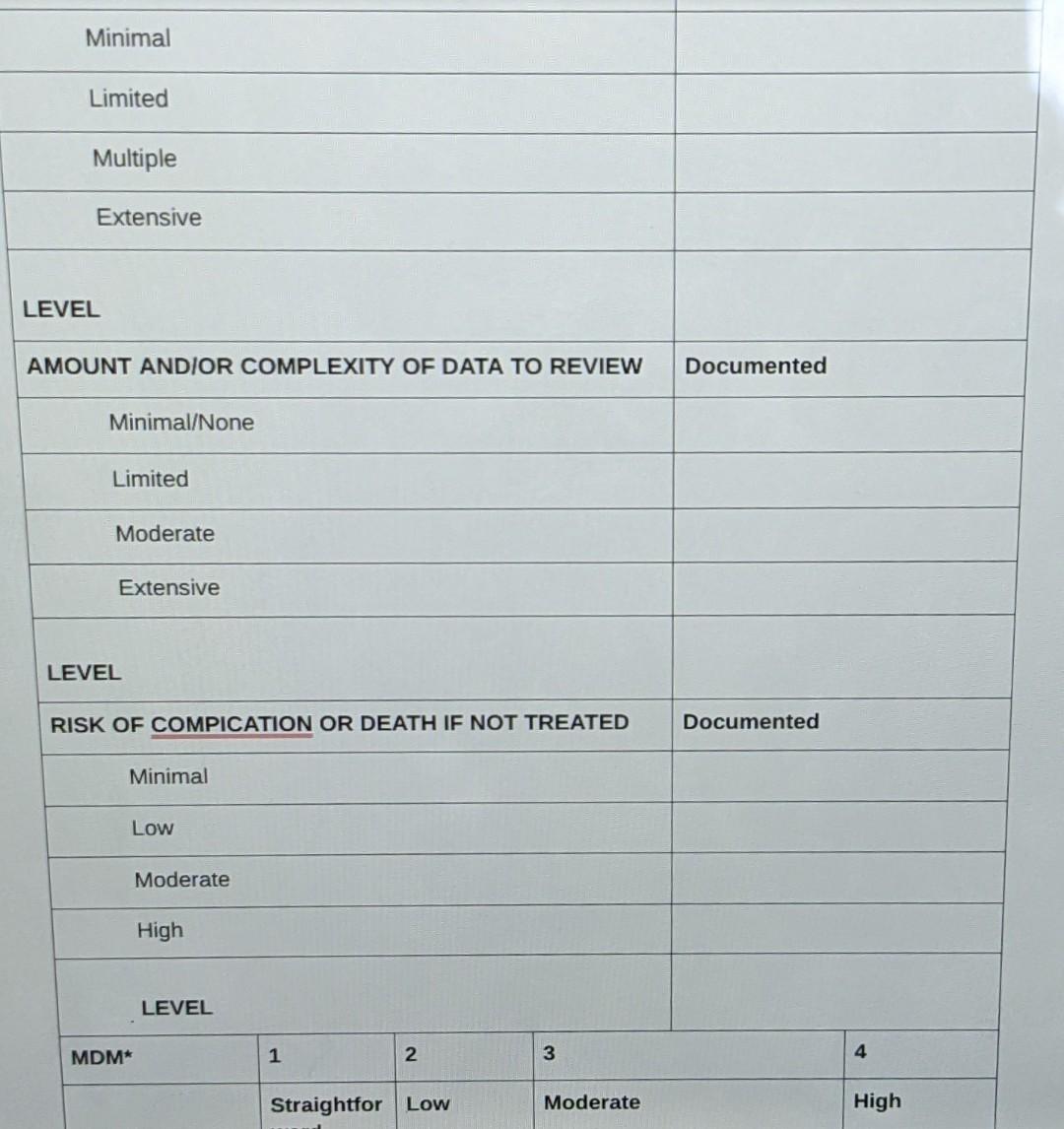
Please fill out the audit form with the informationprovided.