
Make an endorsement to the following case.
Transcribed Image Text from this Question
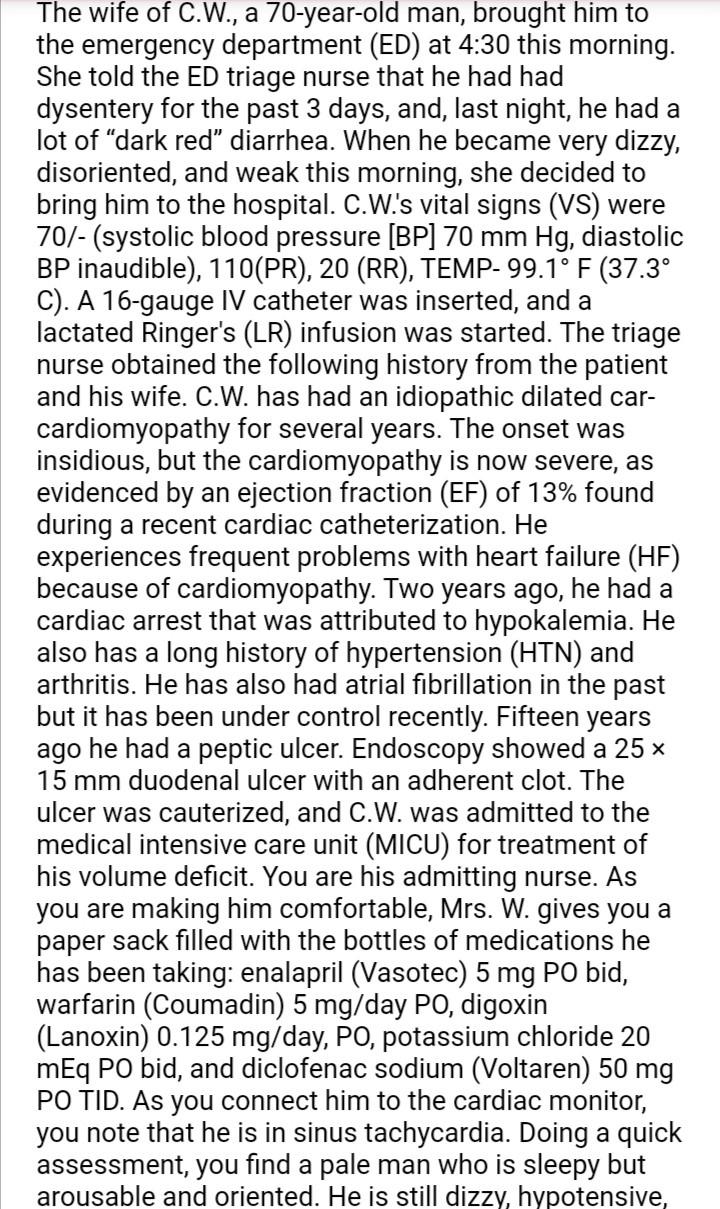
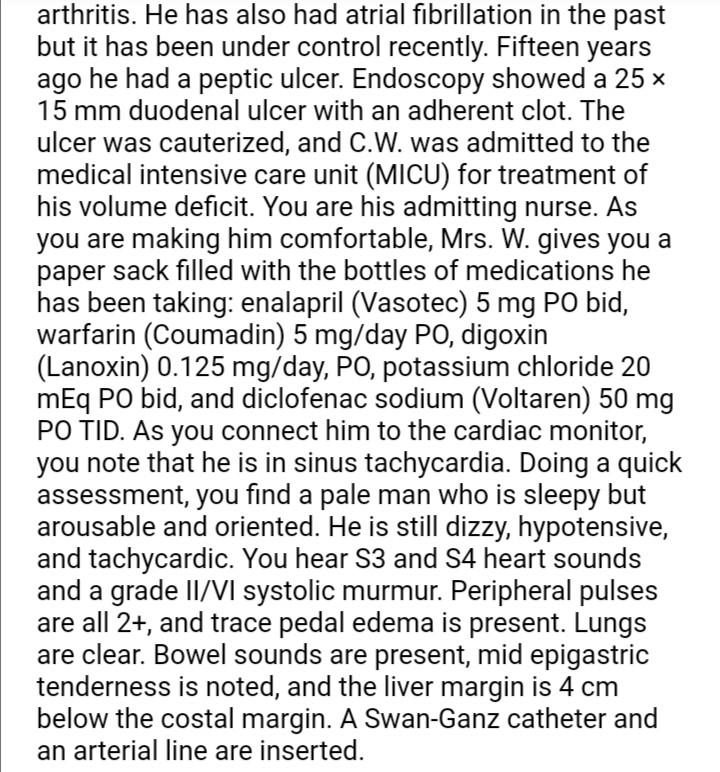
The wife of C.W., a 70-year-old man, brought him to the emergency department (ED) at 4:30 this morning. She told the ED triage nurse that he had had dysentery for the past 3 days, and, last night, he had a lot of “dark red” diarrhea. When he became very dizzy, disoriented, and weak this morning, she decided to bring him to the hospital. C.W.’s vital signs (VS) were 70/- (systolic blood pressure [BP] 70 mm Hg, diastolic BP inaudible), 110(PR), 20 (RR), TEMP-99.1° F (37.3° C). A 16-gauge IV catheter was inserted, and a lactated Ringer’s (LR) infusion was started. The triage nurse obtained the following history from the patient and his wife. C.W. has had an idiopathic dilated car- cardiomyopathy for several years. The onset was insidious, but the cardiomyopathy is no severe, as evidenced by an ejection fraction (EF) of 13% found during a recent cardiac catheterization. He experiences frequent problems with heart failure (HF) because of cardiomyopathy. Two years ago, he had a cardiac arrest that was attributed to hypokalemia. He also has a long history of hypertension (HTN) and arthritis. He has also had atrial fibrillation in the past but it has been under control recently. Fifteen years ago he had a peptic ulcer. Endoscopy showed a 25 x 15 mm duodenal ulcer with an adherent clot. The ulcer was cauterized, and C.W. was admitted to the medical intensive care unit (MICU) for treatment of his volume deficit. You are his admitting nurse. As you are making him comfortable, Mrs. W. gives you a paper sack filled with the bottles of medications he has been taking: enalapril (Vasotec) 5 mg PO bid, warfarin (Coumadin) 5 mg/day PO, digoxin (Lanoxin) 0.125 mg/day, Po, potassium chloride 20 mEq PO bid, and diclofenac sodium (Voltaren) 50 mg PO TID. As you connect him to the cardiac monitor, you note that he is in sinus tachycardia. Doing a quick assessment, you find a pale man who is sleepy but arousable and oriented. He is still dizzy, hypotensive, arthritis. He has also had atrial fibrillation in the past but it has been under control recently. Fifteen years ago he had a peptic ulcer. Endoscopy showed a 25 x 15 mm duodenal ulcer with an adherent clot. The ulcer was cauterized, and C.W. was admitted to the medical intensive care unit (MICU) for treatment of his volume deficit. You are his admitting nurse. As you are making him comfortable, Mrs. W. gives you a paper sack filled with the bottles of medications he has been taking: enalapril (Vasotec) 5 mg PO bid, warfarin (Coumadin) 5 mg/day PO, digoxin (Lanoxin) 0.125 mg/day, PO, potassium chloride 20 mEq PO bid, and diclofenac sodium (Voltaren) 50 mg PO TID. As you connect him to the cardiac monitor, you note that he is in sinus tachycardia. Doing a quick assessment, you find a pale man who is sleepy but arousable and oriented. He is still dizzy, hypotensive, and tachycardic. You hear S3 and 54 heart sounds and a grade II/VI systolic murmur. Peripheral pulses are all 2+, and trace pedal edema is present. Lungs are clear. Bowel sounds are present, mid epigastric tenderness is noted, and the liver margin is 4 cm below the costal margin. A Swan-Ganz catheter and an arterial line are inserted.
(Visited 3 times, 1 visits today)


