
Transcribed Image Text from this Question
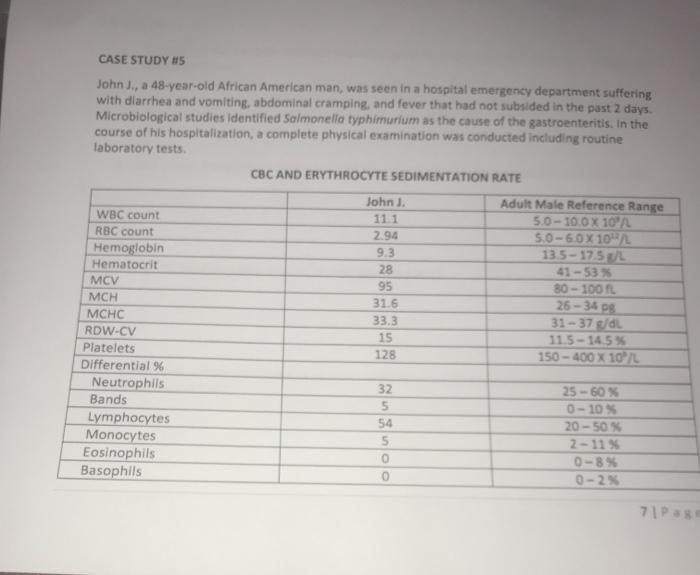
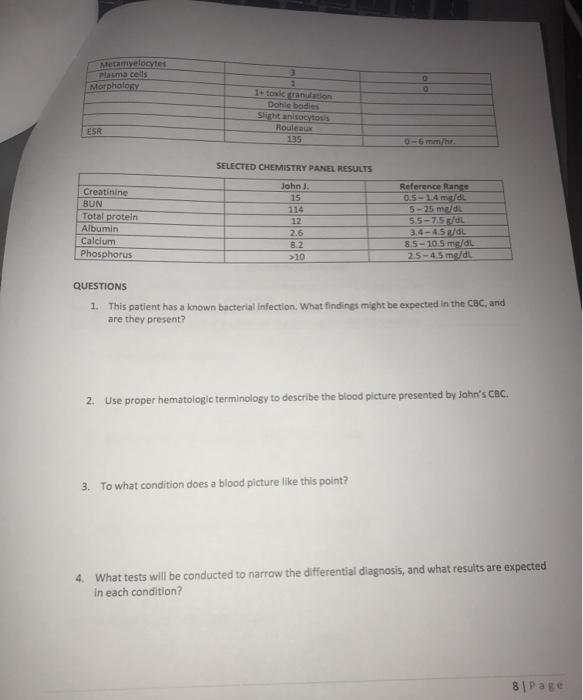
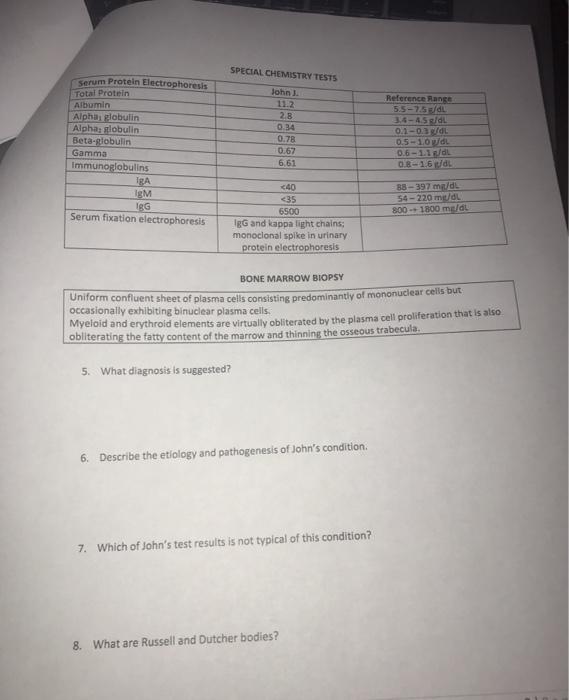
CASE STUDY #15 John J., a 48-year-old African American man, was seen in a hospital emergency department suffering with diarrhea and vomiting, abdominal cramping, and fever that had not subsided in the past 2 days Microbiological studies identified Salmonella typhimurium as the cause of the gastroenteritis. In the course of his hospitalization, a complete physical examination was conducted including routine laboratory tests CBC AND ERYTHROCYTE SEDIMENTATION RATE John Adult Male Reference Range WBC count 111 50 – 100 X 10″ RBC count 2.94 50-60X10/L Hemoglobin 9.3 13.5-17.5 L Hematocrit 28 41 -53 MCV 95 80-100 MCH 31.6 26 – 34 PS MCHC 33.3 31 – 37 di RDW-CV 15 115-1455 Platelets 128 150 – 400 X 10 Differential % Neutrophils 32 25 -60% Bands 5 0 – 10% Lymphocytes 54 20-50 Monocytes 5 2-11% Eosinophils 0-8% Basophils 0 0-2% 713 Metamvelocytes Plasma cells Morphology O 1 1. to cranulation Dohle bodies Sicht an socytos Rouleaux 135 ESR SELECTED CHEMISTRY PANEL RESULTS Creatinine BUN Total protein Albumin Calcium Phosphorus John. 15 114 12 2.6 8.2 >>10 Reference Range 0.5-1.4 mg/dL 5-25 med 5.5-7.5 L 3.4- 4.5 dl 8.5-10 Smed 2.5-4.5 mg/dt QUESTIONS 1. This patient has a known bacterial infection. What findings might be expected in the CBC, and are they present? 2. Use proper hematologic terminology to describe the blood picture presented by John’s CBC. 3. To what condition does a blood picture like this point? 4. What tests will be conducted to narrow the differential diagnosis, and what results are expected in each condition? 8 Page SPECIAL CHEMISTRY TESTS John. serum Protein Electrophoresis Total Protein Albumin Alpha globulin Alpha: slobulin Beta-globulin Gamma Immunoglobulins IgA IgM IgG Serum fixation electrophoresis 28 0.34 0.78 0.67 6,61 Reference Range 5.5-75 3.6- ASSOL 0.1-0.3 L 0.5-10 db 0.6-11/di 0.8-1.6 td 88-397 mild 54-220 ml 800-1800 melal <40 <35 6500 IgG and lappa light chains monoclonal spike in urinary protein electrophoresis BONE MARROW BIOPSY Uniform confluent sheet of plasma cells consisting predominantly of mononuclear cells but occasionally exhibiting binuclear plasma cells. Myeloid and erythroid elements are virtually obliterated by the plasma cell proliferation that is also obliterating the fatty content of the marrow and thinning the osseous trabecula. 5. What diagnosis is suggested? 6. Describe the etiology and pathogenesis of John’s condition. 7. Which of John’s test results is not typical of this condition? 8. What are Russell and Dutcher bodies?
(Visited 3 times, 1 visits today)


