
Transcribed Image Text from this Question
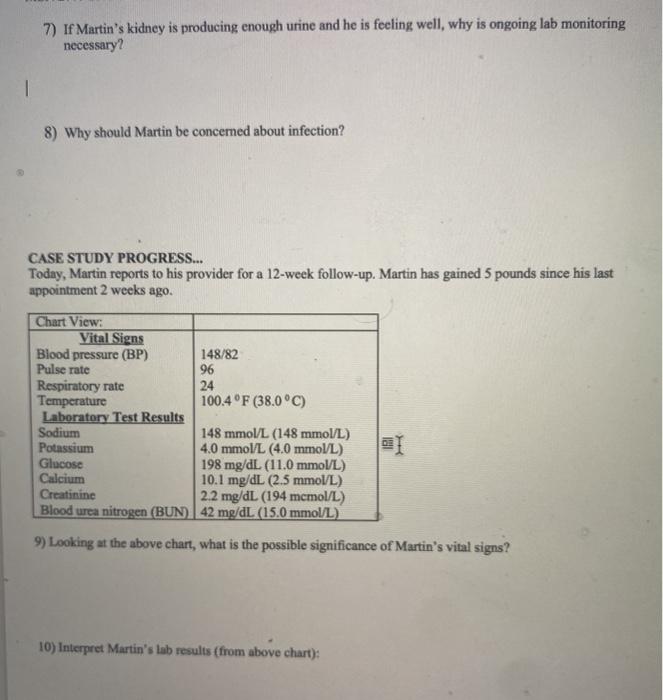
Case Study #1: Martin is a 54-year-old man who lives with his wife and two teenage sons, Martin developed chronic kidney disease 15 years ago after using a drug for migraine headaches that was later shown to cause severe nephrotoxicity. Because of his poor kidney function, he underwent hemodialysis 3 days/week for 3 years before receiving the call that a donor kidney was available him he would soon receive a cadaveric kidney transplant Martin underwent kidney transplantation surgery and did not have any complications while he was hospitalized. Martin’s new kidney was functioning well, and his serum lab values returned to normal. Before his discharge home from the hospital, Martin started immunosuppressive therapy, by taking prednisone and tacrolimus. 1) By what criteria was Martin considered a suitable candidate for a kidney transplant? 2) What histocompatibility studies are usually done before a transplant? Why are they important? 3) Why is Martin receiving prednisone and tacrolimus? I 4) List the priority nursing diagnosis for Martin at this time; 5) Describe an appropriate intervention for this nursing diagnosis: 6) Nume 3 ways in which Martin might have difficulty adjusting after an organ transplant 7) If Martin’s kidney is producing enough urine and he is feeling well, why is ongoing lab monitoring necessary? 8) Why should Martin be concerned about infection? CASE STUDY PROGRESS… Today, Martin reports to his provider for a 12-week follow-up. Martin has gained 5 pounds since his last appointment 2 weeks ago Chart View: Vital Signs Blood pressure (BP) 148/82 Pulse rate 96 Respiratory rate 24 Temperature 100.4 °F (38.0°C) Laboratory Test Results Sodium 148 mmol/L (148 mmol/L) Potassium 4.0 mmol/L (4.0 mmol/L) Glucose 198 mg/dL (11.0 mmol/L) Calcium 10.1 mg/dL (2.5 mmol/L) Creatinine 2.2 mg/dL (194 mcmol/L) Blood urea nitrogen (BUN) 42 mg/dL (15.0 mmol/L) 19 1 9) Looking at the above chart, what is the possible significance of Martin’s vital signs? 10) Interpret Martin’s lab results (from above chart): MSN 277: GROUP CASE STUDY ANALYSIS CASE STUDY PROGRESS… The provider suspects Martin is experiencing acute rejection and orders a renal biopsy, which confirms a diagnosis of acute rejection of the transplanted kidney. 11) Describe the timeframe for acute rejection and briefly explain the pathophysiology of acute rejection. 12) What are the collaborative care options to save the kidney when rejection is present? 13) The healthcare provider adds mycophenolate (CellCept) 1 gram P.O. BID to Martin’s immunosuppressive regimen. How will mycophenolate helt protect Martin’s kidney? 14) Glipizide is prescribed for Martin’s hyperglycemia. Martin asks if this means he is now diabetic. How would you answer him? MSN 277: GROUP CASE STUDY ANALYSIS 15) Martin asks you if this means he is going to lose the kidney and go back on dialysis. How would you respond? 16) How can you best support Martin and his family during this time? 1 CASE STUDY OUTCOME… Martin does not experience any further episodes of acute rejection and within 6 months is able to be on lower doses of immunosuppressive therapy. With the lower level of immunosuppression, his elevated glucose resolves, and he does not develop diabetes. His kidney continues to function well, and he says that despite a few challenges that come with being a post-transplant patient, “I feel better than I have in years.”
(Visited 3 times, 1 visits today)


