
I don’t have more inform
Transcribed Image Text from this Question
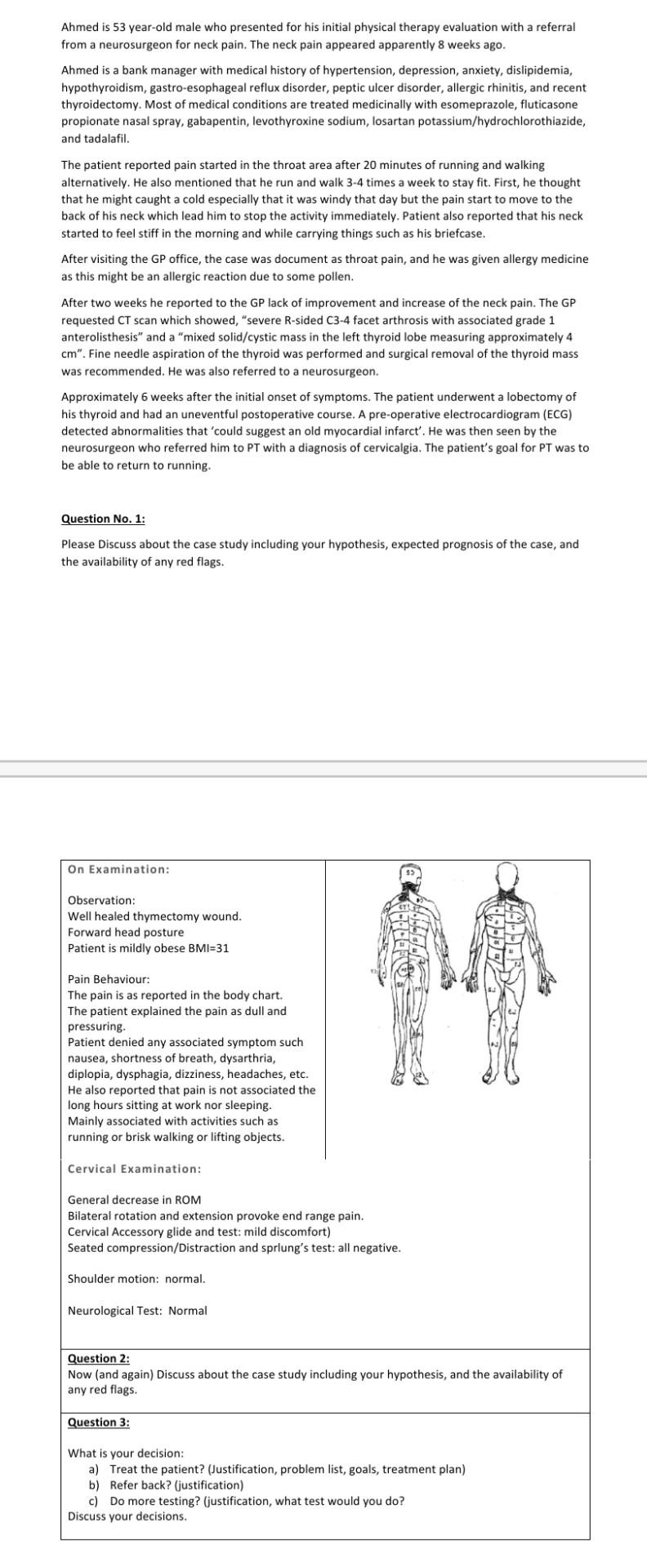
Ahmed is 53 year-old male who presented for his initial physical therapy evaluation with a referral from a neurosurgeon for neck pain. The neck pain appeared apparently 8 weeks ago. Ahmed is a bank manager with medical history of hypertension, depression, anxiety, dislipidemia, hypothyroidism, gastro-esophageal reflux disorder, peptic ulcer disorder, allergic rhinitis, and recent thyroidectomy. Most of medical conditions are treated medicinally with esomeprazole, fluticasone propionate nasal spray, gabapentin, levothyroxine sodium, losartan potassium/hydrochlorothiazide, and tadalafil. The patient reported pain started in the throat area after 20 minutes of running and walking alternatively. He also mentioned that he run and walk 3-4 times a week to stay fit. First, he thought that he might caught a cold especially that it was windy that day but the pain start to move to the back of his neck which lead him to stop the activity immediately. Patient also reported that his neck started to feel stiff in the morning and while carrying things such as his briefcase. After visiting the GP office, the case was document as throat pain, and he was given allergy medicine as this might be an allergic reaction due to some pollen. After two weeks he reported to the GP lack of improvement and increase of the neck pain. The GP requested CT scan which showed, “severe R-sided C3-4 facet arthrosis with associated grade 1 anterolisthesis” and a “mixed solid/cystic mass in the left thyroid lobe measuring approximately 4 cm”. Fine needle aspiration of the thyroid was performed and surgical removal of the thyroid mass was recommended. He was also referred to a neurosurgeon. Approximately 6 weeks after the initial onset of symptoms. The patient underwent a lobectomy of his thyroid and had an uneventful postoperative course. A pre-operative electrocardiogram (ECG) detected abnormalities that ‘could suggest an old myocardial infarct’. He was then seen by the neurosurgeon who referred him to PT with a diagnosis of cervicalgia. The patient’s goal for PT was to be able to return to running. Question No. 1: Please Discuss about the case study including your hypothesis, expected prognosis of the case, and the availability of any red flags. On Examination: Observation: Well healed thymectomy wound. Forward head posture Patient is mildly obese BMI=31 LATES Pain Behaviour: The pain is as reported in the body chart. The patient explained the pain as dull and pressuring. Patient denied any associated symptom such nausea, shortness of breath, dysarthria, diplopia, dysphagia, dizziness, headaches, etc. He also reported that pain is not associated the long hours sitting at work nor sleeping. Mainly associated with activities such as running or brisk walking or lifting objects. Cervical Examination: General decrease in ROM Bilateral rotation and extension provoke end range pain. Cervical Accessory glide and test: mild discomfort) Seated compression/Distraction and sprlung’s test: all negative. Shoulder motion: normal. Neurological Test: Normal Question 2: Now (and again) Discuss about the case study including your hypothesis, and the availability of any red flags. Question 3: What is your decision: a) Treat the patient? (Justification, problem list, goals, treatment plan) b) Refer back? (justification) c) Do more testing? (justification, what test would you do? Discuss your decisions.
(Visited 2 times, 1 visits today)


