
Transcribed Image Text from this Question
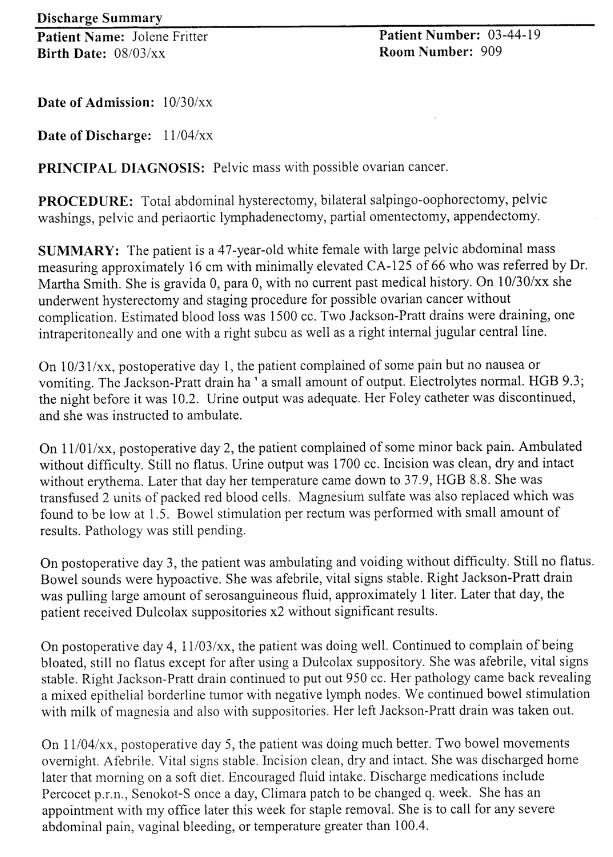
Discharge Summary Patient Name: Jolene Fritter Birth Date: 08/03/xx Patient Number: 03-44-19 Room Number: 909 Date of Admission: 10/30/xx Date of Discharge: 11/04/xx PRINCIPAL DIAGNOSIS: Pelvic mass with possible ovarian cancer. PROCEDURE: Total abdominal hysterectomy, bilateral salpingo-oophorectomy, pelvic washings, pelvic and periaortic lymphadenectomy, partial omentectomy, appendectomy. SUMMARY: The patient is a 47-year-old white female with large pelvic abdominal mass measuring approximately 16 cm with minimally elevated CA-125 of 66 who was referred by Dr. Martha Smith. She is gravida 0, para 0, with no current past medical history. On 10/30/xx she underwent hysterectomy and staging procedure for possible ovarian cancer without complication. Estimated blood loss was 1500 cc. Two Jackson-Pratt drains were draining, one intraperitoneally and one with a right subcu as well as a right internal jugular central line. On 10/31/xx, postoperative day 1, the patient complained of some pain but no nausea or vomiting. The Jackson-Pratt drain ha’a small amount of output. Electrolytes normal. HGB 9.3; the night before it was 10.2. Urine output was adequate. Her Foley catheter was discontinued, and she was instructed to ambulate. On 11/01/xx, postoperative day 2, the patient complained of some minor back pain. Ambulated without difficulty. Still no flatus. Urine output was 1700 cc. Incision was clean, dry and intact without erythema. Later that day her temperature came down to 37.9, HGB 8.8. She was transfused 2 units of packed red blood cells. Magnesium sulfate was also replaced which was found to be low at 1.5. Bowel stimulation per rectum was performed with small amount of results. Pathology was still pending, On postoperative day 3, the patient was ambulating and voiding without difficulty. Still no flatus. Bowel sounds were hypoactive. She was afebrile, vital signs stable. Right Jackson-Pratt drain was pulling large amount of serosanguineous fluid, approximately 1 liter. Later that day, the patient received Dulcolax suppositories x2 without significant results. On postoperative day 4, 11/03/xx, the patient was doing well. Continued to complain of being bloated, still no flatus except for after using a Dulcolax suppository. She was afebrile, vital signs stable. Right Jackson-Pratt drain continued to put out 950 cc. Her pathology came back revealing a mixed epithelial borderline tumor with negative lymph nodes. We continued bowel stimulation with milk of magnesia and also with suppositories. Her left Jackson-Pratt drain was taken out. On 11/04/xx, postoperative day 5, the patient was doing much better. Two bowel movements overnight. Afebrile. Vital signs stable. Incision clean, dry and intact. She was discharged home later that morning on a soft diet. Encouraged Muid intake. Discharge medications include Percocet pr.n., Senokot-S once a day, Climara patch to be changed q. week. She has an appointment with my office later this week for staple removal. She is to call for any severe abdominal pain, vaginal bleeding, or temperature greater than 100.4. 1. 2. 3. What is the diagnosis? What is this patient’s obstetrical history? What operative procedures were performed? What were the results of the pathology specimens? What were the significant events between post-operative day four and five that lead to her being discharged? 4. 5.
(Visited 4 times, 1 visits today)


