

Transcribed Image Text from this Question
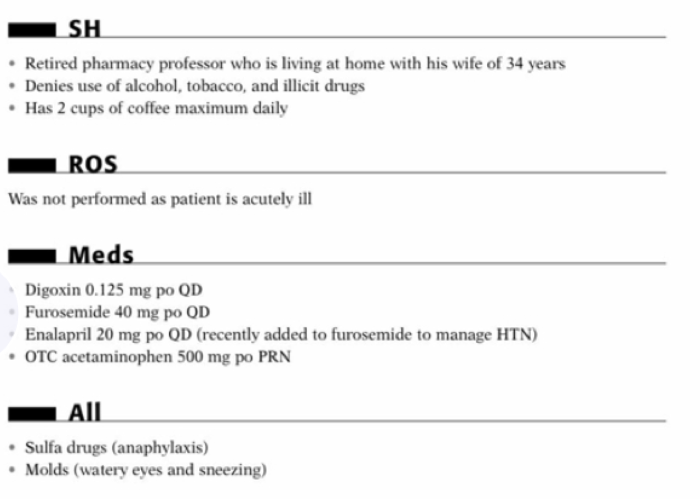
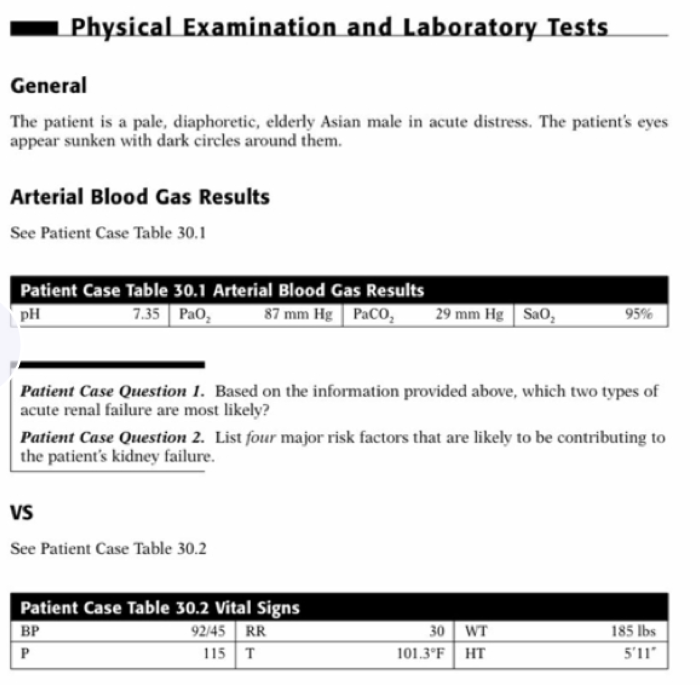
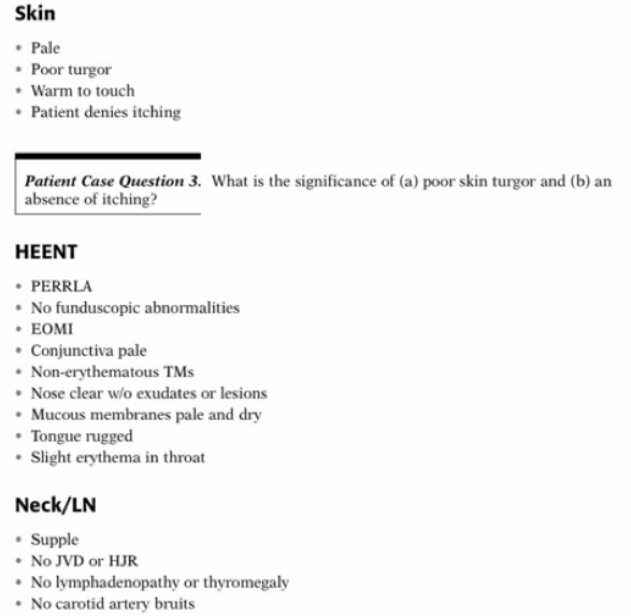
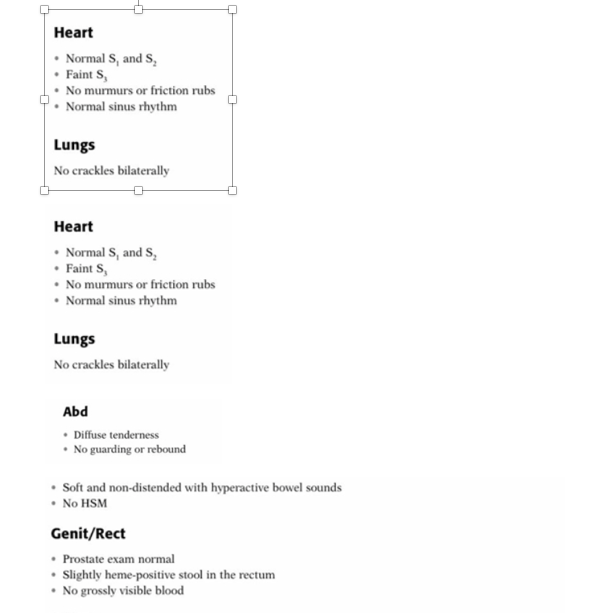
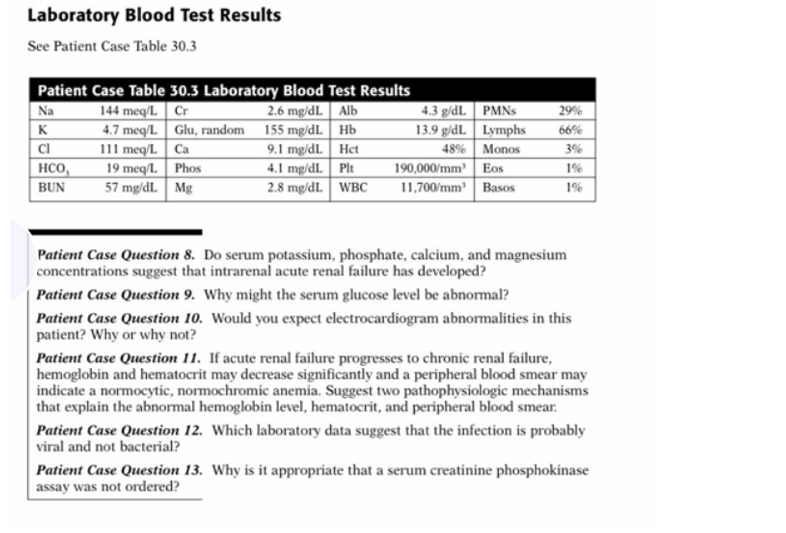
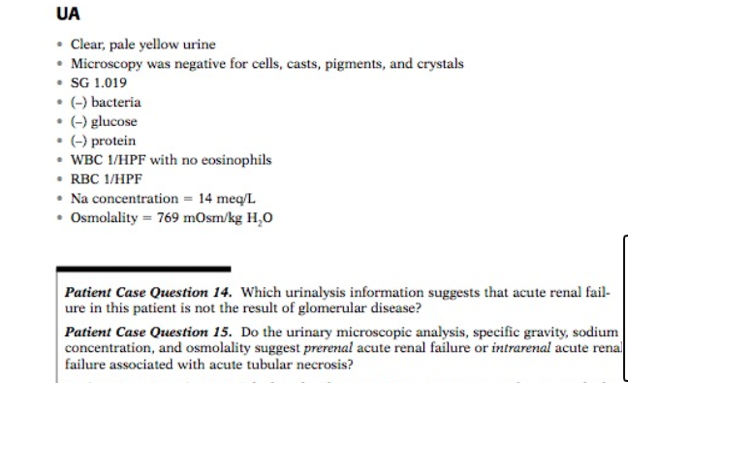
HPI Mr. J.R. is a 73-year-old man, who was admitted to the hospital with clinical manifestations of gastroenteritis and possible renal failure. The patient’s chief complaints are fever, nausea with vomiting and diarrhea for 48 hours, weakness, dizziness, and a bothersome metallic taste in the mouth. The patient is pale and sweaty. He had been well until two days ago, when he began to experience severe nausea several hours after eating two burritos for supper. The burritos had been ordered from a local fast-food restaurant. The nausea persisted and he vomited twice with some relief. As the evening pro- gressed, he continued to feel “very bad” and took some Pepto-Bismol to help settle his stom- ach. Soon thereafter, he began to feel achy and warm. His temperature at the time was 100.5°F. He has continued to experience nausea, vomiting, and a fever. He has not been able to tolerate any solid foods or liquids. Since yesterday, he has had 5-6 watery bowel movements. He has not noticed any blood in the stools. His wife brought him to the ER because he was becoming weak and dizzy when he tried to stand up. His wife denies any recent travel, use of antibiotics, laxatives, or excessive caffeine, or that her husband has an eating disorder. PMH HTN X 14 years • Post-AMI X 10 years Heart failure x 8 years • No known renal disease or DM • Osteoarthritis x 5 years • DVT at age 61, treated with anticoagulants for 1 year FH Father died at age 50 from AMI Mother has type 2 DM • Has two brothers, both living, with no known medical problems Has two sons without medical problems SH • Retired pharmacy professor who is living at home with his wife of 34 years • Denies use of alcohol, tobacco, and illicit drugs • Has 2 cups of coffee maximum daily ROS Was not performed as patient is acutely ill Meds Digoxin 0.125 mg po QD Furosemide 40 mg po QD Enalapril 20 mg po QD (recently added to furosemide to manage HTN) • OTC acetaminophen 500 mg po PRN All • Sulfa drugs (anaphylaxis) Molds (watery eyes and sneezing) Physical Examination and Laboratory Tests General The patient is a pale, diaphoretic, elderly Asian male in acute distress. The patient’s eyes appear sunken with dark circles around them. Arterial Blood Gas Results See Patient Case Table 30.1 Patient Case Table 30.1 Arterial Blood Gas Results PH 7.35 Pao, 87 mm Hg PaCO, 29 mm Hg | Sao, 95% Patient Case Question 1. Based on the information provided above, which two types of acute renal failure are most likely? Patient Case Question 2. List four major risk factors that are likely to be contributing to the patient’s kidney failure. VS See Patient Case Table 30.2 Patient Case Table 30.2 Vital Signs BP 92/45 RR P 115T 30 WT 101.3°F HT 185 lbs 5’11” Skin • Pale • Poor turgor • Warm to touch • Patient denies itching Patient Case Question 3. What is the significance of (a) poor skin turgor and (b) an absence of itching? HEENT • PERRLA • No funduscopic abnormalities • EOMI • Conjunctiva pale • Non-erythematous TMs • Nose clear w/o exudates or lesions • Mucous membranes pale and dry • Tongue rugged • Slight erythema in throat Neck/LN • Supple • No JVD or HJR • No lymphadenopathy or thyromegaly • No carotid artery bruits Heart • Normal S, and S, • Faints • No murmurs or friction rubs • Normal sinus rhythm Lungs No crackles bilaterally Heart • Normal S, and S, • Faint • No murmurs or friction rubs • Normal sinus rhythm Lungs No crackles bilaterally Abd • Diffuse tenderness • No guarding or rebound • Soft and non-distended with hyperactive bowel sounds • No HSM Genit/Rect • Prostate exam normal Slightly heme-positive stool in the rectum • No grossly visible blood . . MS/Ext • Normal muscle strength bilaterally • No CCE • Peripheral pulses weak at 1+ bilaterally • Patient denies any muscle tenderness Neuro A&OX 3 • CNs intact • Motor function—no focal weakness • Slightly decreased patellar reflex, otherwise normal reflexes • Normal coordination and gait Patient Case Question 7. What is the significance of the neurological findings in this patient? Laboratory Blood Test Results See Patient Case Table 30.3 29% 66% Patient Case Table 30.3 Laboratory Blood Test Results Na 144 meq/L Cr 2.6 mg/dl Alb 4.3 g/dL PMNS K 4.7 meq/L. Glu, random 155 mg/dl. Hb 13.9 g/dL. Lymphs CI 111 meq/L Ca 9.1 mg/dl. Het 48% Monos HCO , 19 meq/l. Phos 4.1 mg/dL Plt 190,000/mm Eos BUN 57 mg/dl. Mg 2.8 mg/dL. WBC 11,700/mm Basos 3% Patient Case Question 8. Do serum potassium, phosphate, calcium, and magnesium concentrations suggest that intrarenal acute renal failure has developed? Patient Case Question 9. Why might the serum glucose level be abnormal? Patient Case Question 10. Would you expect electrocardiogram abnormalities in this patient? Why or why not? Patient Case Question 11. If acute renal failure progresses to chronic renal failure, hemoglobin and hematocrit may decrease significantly and a peripheral blood smear may indicate a normocytic, normochromic anemia. Suggest two pathophysiologic mechanisms that explain the abnormal hemoglobin level, hematocrit, and peripheral blood smear. Patient Case Question 12. Which laboratory data suggest that the infection is probably viral and not bacterial? Patient Case Question 13. Why is it appropriate that a serum creatinine phosphokinase assay was not ordered? UA • Clear, pale yellow urine • Microscopy was negative for cells, casts, pigments, and crystals • SG 1.019 • (-) bacteria • (-) glucose • (-) protein • WBC 1/HPF with no eosinophils • RBC 1/HPF . Na concentration = 14 meq/L • Osmolality = 769 mOsm/kg H,0 Patient Case Question 14. Which urinalysis information suggests that acute renal fail- ure in this patient is not the result of glomerular disease? Patient Case Question 15. Do the urinary microscopic analysis, specific gravity, sodium concentration, and osmolality suggest prerenal acute renal failure or intrarenal acute renal failure associated with acute tubular necrosis?
(Visited 4 times, 1 visits today)


