
Assit w/simulator prep assignments: 1, 2, 3 (1-4)
Transcribed Image Text from this Question
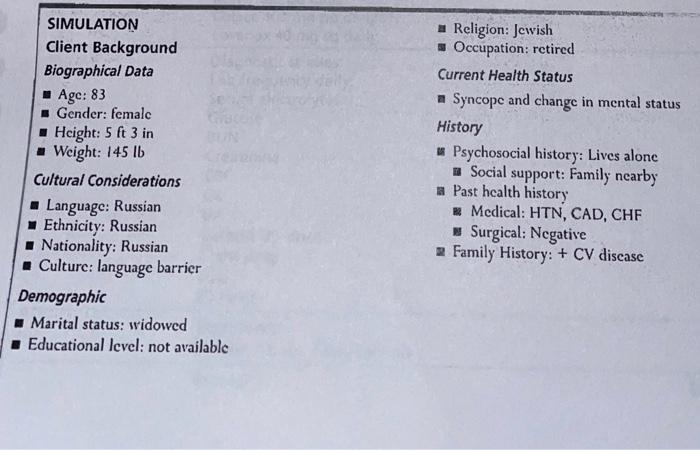
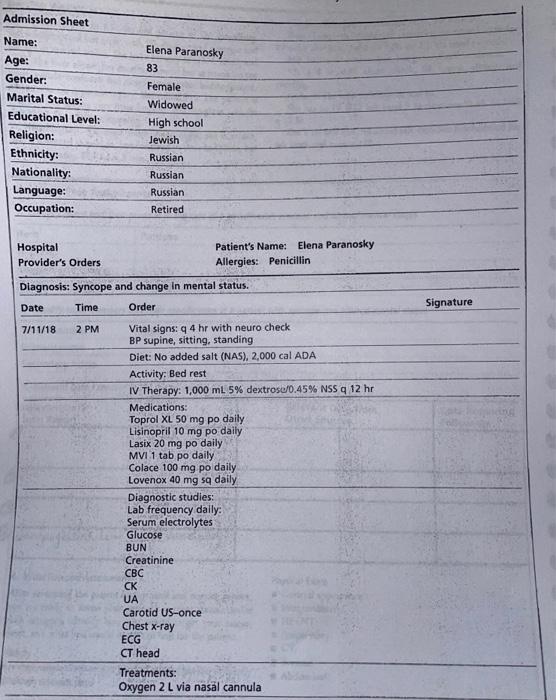
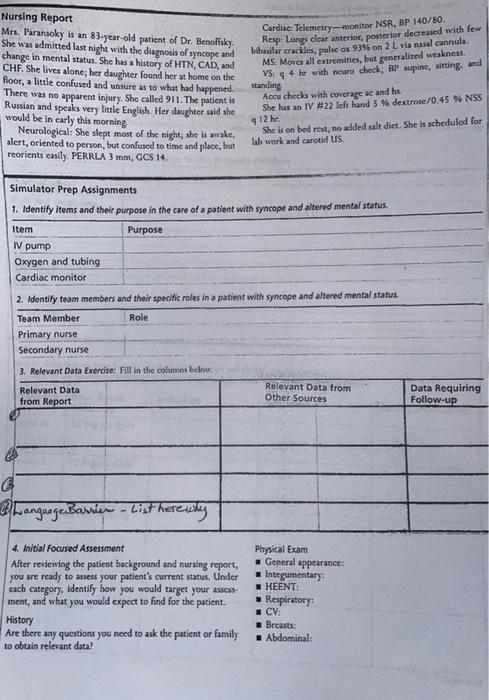
SIMULATION Client Background Biographical Data Age: 83 Gender: femalc Height: 5 ft 3 in Weight: 145 lb Cultural Considerations Language: Russian Ethnicity: Russian Nationality: Russian Culture: language barrier Demographic Marital status: widowed Educational level: not available Religion: Jewish Occupation: retired Current Health Status Syncope and change in mental status History Psychosocial history: Lives alone Social support: Family nearby * Past health history – Medical: HTN, CAD, CHF Surgical: Negative Family History: + CV discase Admission Sheet Elena Paranosky Name: Age: Gender: Marital Status: Educational Level: Religion: Ethnicity: Nationality: Language: Occupation: 83 Female Widowed High school Jewish Russian Russian Russian Retired Hospital Patient’s Name: Elena Paranosky Provider’s Orders Allergies: Penicillin Diagnosis: Syncope and change in mental status. Date Time Order Signature 7/11/18 2 PM Vital signs: 9 4 hr with neuro check BP supine, sitting, standing Diet: No added salt (NAS), 2,000 cal ADA Activity: Bed rest IV Therapy: 1,000 ml 5% dextrose/0.45% NSS 12 hr Medications: Toprol XL 50 mg po daily Lisinopril 10 mg po daily Lasix 20 mg po daily MVI 1 tab po daily Colace 100 mg po daily Lovenox 40 mg sa daily Diagnostic studies: Lab frequency dally: Serum electrolytes Glucose BUN Creatinine CBC CK UA Carotid US-once Chest x-ray ECG CT head Treatments: Oxygen 2 L via nasal cannula Nursing Report Mrs. Parasoky is an 83-year-old patient of Dr. Benoflíky, She was admitted last night with the diagnosis of syncope and change in mental status. She has a history of HTN, CAD, and CHF. She lives alone; her daughter found her at home on the floor, a little confused and unsure as to what had happened. There was no apparent injury. She called 911. The patient is Russian and speaks very little English. Her daughter said she would be in early this morning Neurological: She slept most of the night, she is swake, alert, oriented to person, but confused to time and place, but reorients easily, PERRLA 3 mm, GCS 14. Cardiac Telemetry-monitor NSR, BP 140/80 Resp Lungi clear anterior, posterior decreased with few biballar crackles, pulse ox 93% on 2 L ria nasal cannula. MS: Moves all extremities, but generalized weakness. VS: 4 hr with scuro check, RP supine, sitting, and Accu checks with coverage ac and he She has an IV #22 left hand 5 % dextrose/0.45 % NSS She is on bed rest, no added salt diet. She is scheduled for lab work and carotid us standing 9 12 h Simulator Prep Assignments 1. Identity items and their purpose in the care of a patient with syncope and altered mental status Item Purpose IN pump Oxygen and tubing Cardiac monitor 2. Identify team members and their specific roles in a patient with syncope and altered mental status Team Member Role Primary nurse Secondary nurse 3. Relevant Data Exercise: Fill in the columns below Relevant Data from Report Rolevant Data from Other Sources Data Requiring Follow-up Language Barrier • List here why 4 Initial focused Assessment After reviewing the patient background and nursing report, you are ready to assess your patient’s current status. Under cach category, identify how you would target your assess ment, and what you would expect to find for the patient. History Are there any questions you need to ask the patient or family to obtain relevant data? Physical Exam General appearance: Integumentary HEENT: Respiratory CV: Breasts: Abdominal:
(Visited 4 times, 1 visits today)


