

Transcribed Image Text from this Question
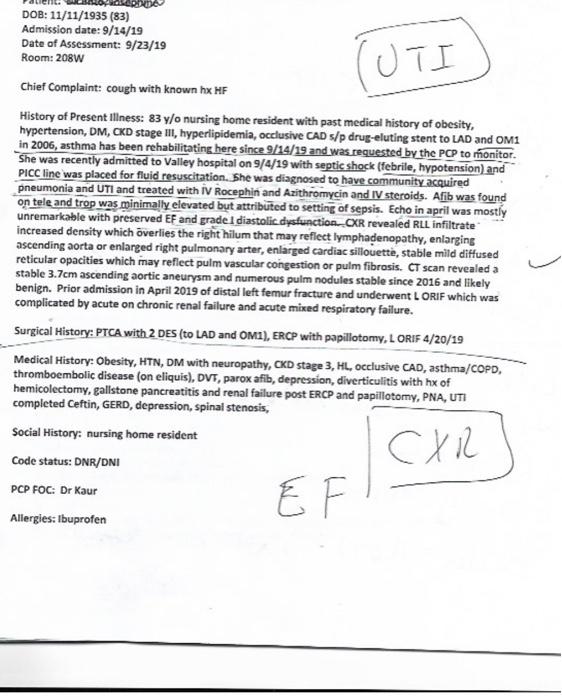
TUTI 프 DOB: 11/11/1935 (83) Admission date: 9/14/19 Date of Assessment: 9/23/19 Room: 208W Chief Complaint: cough with known hx HF History of Present illness: 83 y/o nursing home resident with past medical history of obesity, hypertension, DM, CKD stage III, hyperlipidemia, occlusive CAD s/p drug-eluting stent to LAD and OMI in 2006, asthma has been rehabilitating here since 9/14/19 and was requested by the PCP to monitor. She was recently admitted to Valley hospital on 9/4/19 with septic shock (febrile, hypotension) and PICC line was placed for fluid resuscitation. She was diagnosed to have community acquired pneumonia and UTI and treated with IV Rocephin and Azithromycin and IV steroids. Afib was found on tele and trop was minimally elevated but attributed to setting of sepsis. Echo in april was mostly unremarkable with preserved EF and grade 1 diastolic dysfunction.OXR revealed RLL infiltrate increased density which overlies the right hilum that may reflect lymphadenopathy, enlarging ascending aorta or enlarged right pulmonary arter, enlarged cardiac sillouette, stable mild diffused reticular opacities which may reflect pulm vascular congestion or pulm fibrosis. CT scan revealed a stable 3.7cm ascending aortic aneurysm and numerous pulm nodules stable since 2016 and likely benign. Prior admission in April 2019 of distal left femur fracture and underwent LORIF which was complicated by acute on chronic renal failure and acute mixed respiratory failure. Surgical History: PTCA with 2 DES (to LAD and OMI), ERCP with papillotomy, LORIF 4/20/19 Medical History: Obesity, HTN, DM with neuropathy, CKD stage 3, HL, occlusive CAD, asthma/COPD, thromboembolic disease (on eliquis), DVT, parox afib, depression, diverticulitis with hx of hemicolectomy, gallstone pancreatitis and renal failure post ERCP and papillotomy, PNA, UTI completed Ceftin, GERD, depression, spinal stenosis, Social History: nursing home resident Code status: DNR/DNI PCP FOC: Dr Kaur CXR EF Allergies: Ibuprofen This patient also has a high RDW what is a RDW and why is it high when the rbc hemoglobin and Hemtocrit are low? +
(Visited 2 times, 1 visits today)


